Adult measles with a butterfly rash-like appearance
Published Web Location
https://doi.org/10.5070/D32dx685hcMain Content
Letter: Adult measles with a butterfly rash-like appearance
Daisuke Tsuruta1, Hiromi Kobayashi1, Ichiro Kurokawa2, Masamitsu Ishii1, Katsuhiro E Takekawa3
Dermatology Online Journal 16 (3): 16
1. Department of Dermatology, Osaka City University Graduate School of Medicine, Osaka, Japan. dtsuruta@med.osaka-cu.ac.jp2. Department of Dermatology, Mie University Medical School, Mie, Japan
3. Takekawa Clinic, Osaka, Japan
Abstract
Butterfly rash is characterized by symmetrical erythema and erythematous papules and plaques grouped on the bilateral cheeks and nose, commonly found in lupus erythematosus. Measles is a highly contagious viral disease, characterized by high fever, cough, coryza, conjunctivitis, and Koplik spots, which precede generalized maculo-papular rashes. We report an adult case of measles, accompanied by butterfly rash. A 20-year-old woman came to our hospital with a butterfly rash-like eruption on the face, high fever, and arthralgia. The eruption had appeared on the nose and both cheeks three days before admission. The oral mucosa was not involved. On the basis of the three criteria for a diagnosis of lupus eruthematosus, we first made a tentative diagnosis of lupus eruthematosus and performed blood tests. However, anti-DNA antibodies, scl-70, anti-Ro and La, anti-Sm and rheumatoid factor were all negative. Two days after admission, a Koplik macule appeared along with multiple erythematous macules and papules that were scattered through the trunk. Laboratory tests were positive for anti-measles immunoglobulin M and G. Therefore, we reached a diagnosis of measles. Within a week, all of the clinical symptoms disappeared. Physicians should be aware that, in rare cases, measles may present with a butterfly-like rash.
Introduction
Butterfly rash is characterized by symmetrical erythema and erythematous papules and plaques grouped on the bilateral cheeks and nose. It is associated with collagen vascular diseases such as lupus erythematosus, dermatomyositis, or Sjögren disease [1]. Measles is a highly contagious and acute viral disease, which mainly affects children [2, 3]. It is characterized by high fever, cough, coryza, conjunctivitis, and Koplik spots, which precede a generalized florid maculo-papular eruption [2, 3]. Recently, we observed an adult case of measles, accompanied by high fever, arthralgia, and butterfly rash with symmetrical erythema without any cough, coryza, conjunctivitis, or Koplik spots at the time of first presentation. Our original diagnosis was systemic lupus erythematosus, with a final diagnosis of measles in the young adult.
Case report
 |  |
| Figure 1a | Figure 1b |
|---|---|
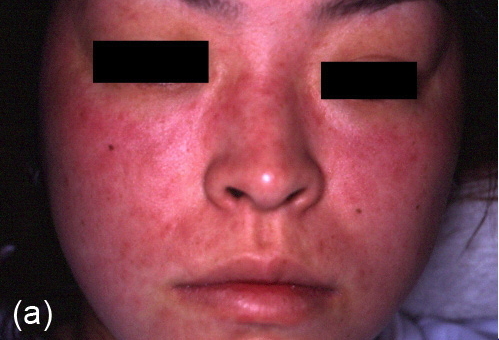
| Figure 1a. Edematous erythematous macules on both eyelids, cheeks, and the nose. Note the coalescence of erythema from the
cheek to nose. Figure 1b. No Koplik spots were detected at first presentation. | |
A 20-year-old woman came to our hospital with a cutaneous eruption on the face. She also presented with a 3-day history of high fever, temperature of 38.5°C, and arthralgia. The eruption had appeared on the nose and both cheeks 3 days before admission. Physical examination revealed slightly edematous erythematous papules on the nose and both cheeks, with a butterfly-like appearance (Figure 1a); the oral mucosa was not involved (Figure 1b). On the basis of the three criteria for a diagnosis of lupus erythematosus [4], we first made a tentative diagnosis of lupus erythematosus and performed blood tests. However, tests that are particularly specific for collagen vascular diseases, including antinuclear antibody, anti-DNA antibodies, scl-70, anti-Ro and La, anti-Sm, and rheumatoid factor were all negative. Complete blood count, blood chemistry, immunoglobulins, creatine kinase, complement, C-reactive protein, and erythrocyte sedimentation rate were negative.
She had not been vaccinated for measles throughout her life. However, two days after admission, a Koplik macule appeared, multiple erythematous macules and papules developed extensively over the trunk, and laboratory tests were positive for anti-measles immunoglobulin M and G (IgM: 6.60 IU/ml (normal<0.8), IgG: 20 IU/ml (normal<4.0).
Histopathological findings from the affected cheek showed perivascular infiltration primarily comprising lymphocytes. We reached a diagnosis of measles on the basis of the positive test for measles IgM associated with fever, although the presentation was atypical. Within a week, the butterfly rash, oral symptoms, and maculo-papular eruption on the trunk disappeared leaving mild hyperpigmentation; the anti-measles IgM decreased to within the normal range. Therefore, she was discharged from the hospital.
Discussion
In this case, the diagnosis of measles was made on the basis of the positive test for the immunoglobulin M associated with measles. However, the clinical morphology was quite uncharacteristic and exhibited a butterfly rash. Butterfly rash is one of the most typical clinical features of lupus erythematosus, but several disorders show butterfly-like eruptions, such as dermatomyositis, Sjögren syndrome, erythema multiforme, photosensitive dermatitis, scarlet fever, erythema infectiosum, drug eruption, pellagra, Sweet disease, Bloom syndrome, Hartnup syndrome, Cockayne syndrome, rosacea, eosinophilic pustular folliculitis, or eczema [1, 5]. We did not initially consider measles, because there had been no reports of measles with butterfly rash and this disease is now quite uncommon. The number of reported measles cases has declined from 763,094 in 1958 to fewer than 150 cases reported per year since 1997 in the U.S. [6]. Moreover, an estimated 74 percent reduction in mortality resulting from measles was achieved between 2000 and 2007 in the US [7]. However, physicians should be aware that, in rare cases, measles may present with a butterfly-like rash. If appropriate antibody tests are not performed in such cases, the correct diagnosis of measles will not be made.
References
1. Dreizen S, The butterfly rash and the malar flush. What diseases do these signs reflect? Postgrad Med, 1991. 89(1): p. 225-8, p. 233-4. [PubMed]2. Manikkavasagan G, Ramsay M, Protecting infants against measles in England and Wales: a review. Arch Dis Child, 2009. 94(9): p. 681-5. [PubMed]
3. Naniche D, Human immunology of measles virus infection. Curr Top Microbiol Immunol, 2009. 330: p. 151-71. [PubMed]
4. Hochberg MC, Updating the American college of rheumatology revised criteria for the classification of systemic lupus erythematosus. Arthritis Rheum, 1997. 40 (9): p. 1725-34. [PubMed]
5. Tsunemi Y, Saeki H, Ihn H, Tamaki K, Eosinophilic pustular folliculitis with a butterfly rash-like distribution. Dermatology, 2004. 208 (3): p. 229-30. [PubMed]
6. Orenstein WA, Papania MJ, Wharton ME, Measles elimination in the United States. J Infect Dis, 2004.189 (Suppl 1): p. S1-3. [PubMed]
7. Plemper RK, Snyder JP, Measles control—can measles virus inhibitors make a difference? Curr Opin Investig Drugs, 2009. 10 (8): p. 811-20. [PubMed]
© 2010 Dermatology Online Journal